In all the years I’ve spent as a journalist, I can think of stories of ASHAs (Accredited Social Health Activist) from almost every state I’ve worked in.
In the thick of conflict-reporting in Manipur, I met an ASHA worker who, for more than a year, spent her own money to ensure that immunisation happened in a tribal district that was completely cut off from regular medical supplies.
In the midst of an increase in Japanese Encephalitis deaths in the Malkangiri district of Chhattisgarh, I met an ASHA worker who spoke the truth about why infants were dropping dead in the district. A tribal woman herself, she spoke at length about the deep-rooted apathy against tribals in Orissa and the corruption within the Integrated Child Development Services (ICDS) that prevented the poorest communities from accessing primary healthcare and basic nutrition, resulting in lowered immunity among newborns.
During the Covid-19 pandemic, every district I visited in Tamil Nadu had ASHA workers out on the street every day, checking on the symptoms of those in their villages and ensuring timely medical help.
My colleagues from across the country reported on how these healthcare workers were shields against the virus, for their communities.
These are stories that would fit right into the trope of superhero films, where a man emerges from nowhere and saves a world hurtling towards an unimaginable calamity. But here, the ‘heroes’ are women from across the country. There is no thrilling entry; these women are already present, and probably from your neighbourhood. Our familiarity with them — or patriarchy — is one among the many reasons they will never be called ‘heroes’ and receive only the double burden of being women workers.
This group, which has consistently been serving primary healthcare to India’s most underrepresented people and pulling the country through one health scare after the other, have now taken it upon themselves to demand what is due: recognition and fair pay as healthcare workers.
In 1978, the Alma-Ata Declaration led by WHO-UNICEF concluded that focussing on primary healthcare through community health workers is critical to achieving an acceptable level of health throughout the world.
Over the next couple of decades, South Asian governments carved out a role for the largest pool of unemployed people accessible to the state — unmarried women — to work in lower-income communities, villages and the neighbourhoods they belonged to.
These women were publicly identified as ‘volunteers’, paving the way for a system that relied almost entirely on the caregiver ecosystem — with its patriarchal foundations in which the role of women is not just undervalued, but barely considered work.
Most ASHA workers remain underpaid and the labour force at the centre of this organisation are women, many lower-caste; a demographic whose work remains historically undervalued. In this, they join the ranks of conservancy workers, domestic workers, agricultural workers and the thousands of other women in the informal and formal workforce, who are continuously kept away from a fair wage.
This is the story of the longest-ever indefinite day-and-night strike led by women in India’s history. At its centre were hundreds of ASHA workers under KAHWA (Kerala ASHA Health Workers’ Association), who pushed not just Kerala (where the strike was located), but the entire country to sit up and take notice.
Our protagonist is a leader who emerged during this strike, like many others. Her name is Rosamma. One walk through her town with her, and like every other person who passes by and stops to talk, you might start calling her “Rosamma Chechi” too.
***
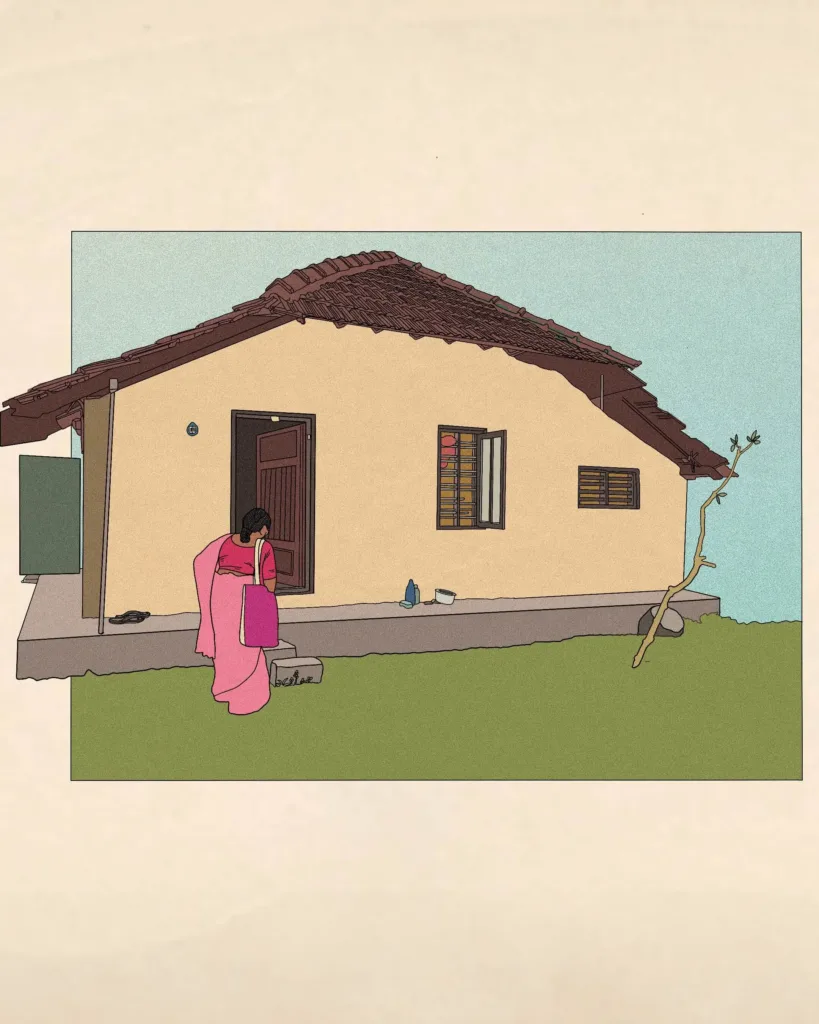
An eerie silence surrounded us as we waited at Yashoda’s door, concern writ large on Rosamma Chechi’s face. The house wore a dilapidated look, enveloped by the smell of moss and abandonment.
Rosamma Chechi walked into the house and instantly spotted Yashoda, seated at the far end, adjacent to the kitchen. It took Yashoda a minute or two to acknowledge us, but as soon as she recognised Rosamma Chechi, her eyes started to well up. Chechi, meanwhile, had walked into the kitchen, asking how long the pot of rice had been on the boil.
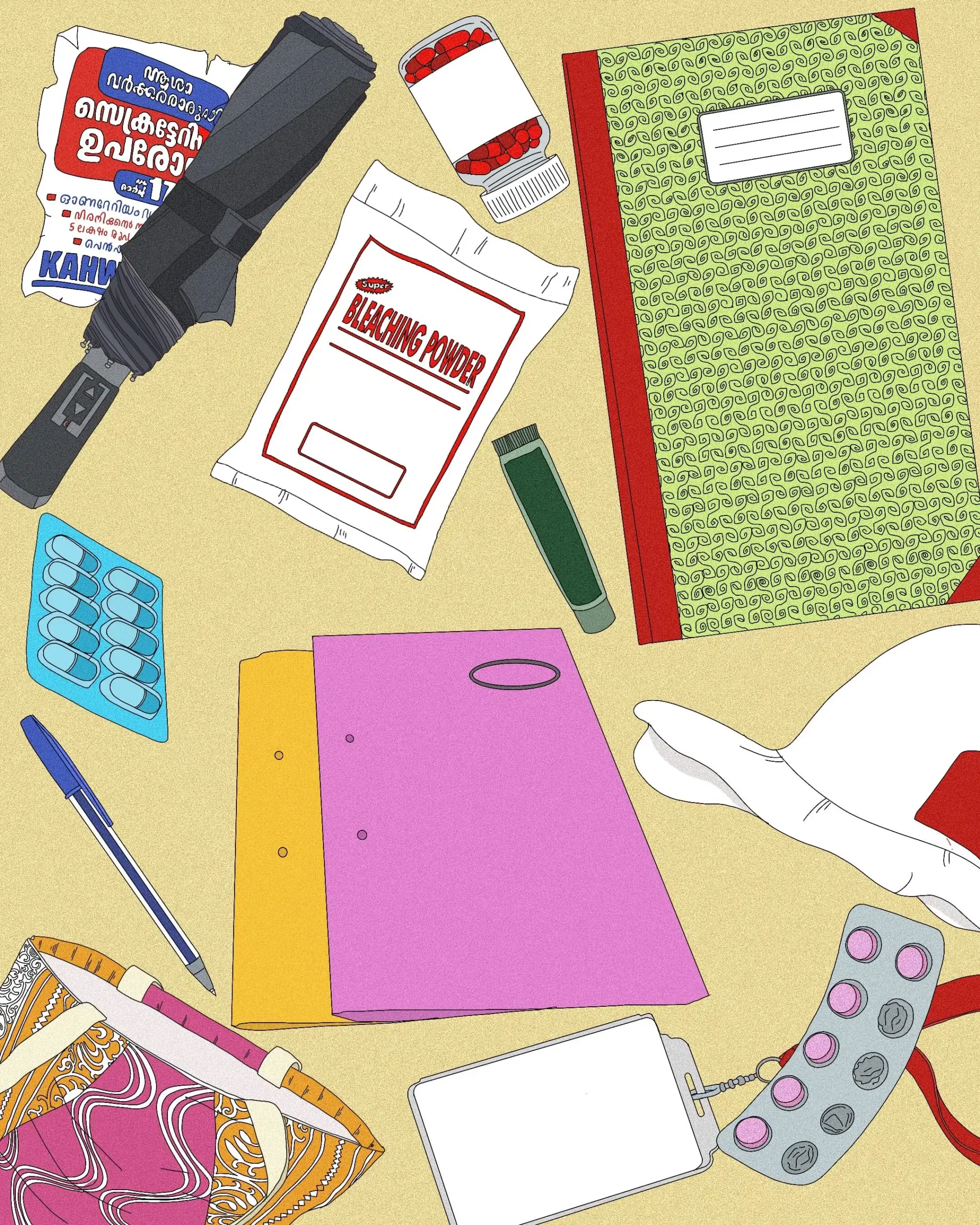
Yashoda seemed to ignore her, distracted, almost like it was her only escape from Chechi’s questions. From the kitchen, Chechi made her way into Yashoda’s bedroom, asking one question after the other, and finally emerged with a polythene bag. She fished out a diary and a paper bag of tablets, and gave a loud gasp.
“You’ve not taken any of these tablets!” she said to Yashoda. By now, Yashoda had stopped making any eye contact with either of us and had moved on to looking out of the doorway.
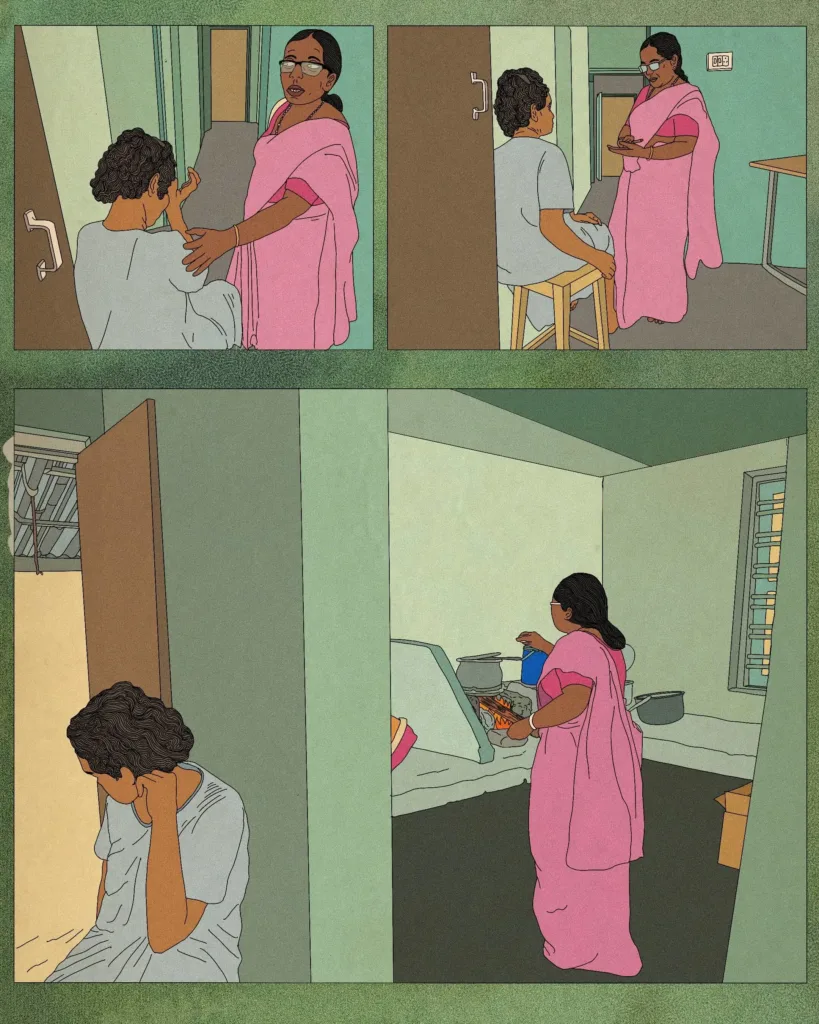
“Look at me! What’s happened?” shouted Rosamma Chechi.
“I am in pain,” replied Yashoda.
She slowly lifted her nightie to show us her knee, which was swollen up and twice the size of her other knee. Holding back tears, she told Chechi that she had slipped and had a fall the previous week. Rosamma Chechi paused briefly before reaching into her bag to fish out a tube of pain-relief ointment, which she told Yashoda to apply on the swollen area.
“But if you don’t take your tablets, you won’t get better,” she reprimanded. “You need to take your tablets, Yashoda!”
“I will try, but…” Yashoda trailed off.
Yashoda had suffered a stroke in 2017, which severely affected her brain function and restricted her speech and movement. Periodic visits from Rosamma Chechi are probably the only form of care she receives.
Yashoda is the mother of two daughters, both of whom are married with children, but according to Rosamma Chechi their husbands don’t want them to visit their mother. So Yashoda continues to live at the house where she raised her children, who no longer want to — or can — visit her.

As a state with an ageing population, Kerala’s need for palliative social care, especially for older people suffering from serious ailments, is only going to rise in the future, as it is also a state that is heavily migratory.
Among the people Rosamma Chechi visited, it was obvious who had the privilege of being cared for. While very few of the older patients had people to care for them, many of the younger ones, especially the men, had caregivers; mothers, sisters or wives. In the case of older women like Yashoda, their children were either living elsewhere because they were married, or living and working outside the country with their families.
This means many of the patients that Rosamma Chechi checks on are senior citizens who have been left to take care of themselves, even if they are not in a position to do so. For at least half of them — unable to afford either caregivers or hospital visits — Rosamma Chechi is their only access to primary healthcare.

The reason for the creation of the ASHA role under the National Rural Health Mission (NRHM) was precisely this: to centre primary healthcare, as decided at the Alma-Ata conference and create a workforce to address challenges that crop up at the panchayat level. The approach was designed to convey that health is a critical right for all citizens and the role of the government is to ensure that such a right is taken to the doorstep of every citizen.
The goals that were set when the first batch of ASHAs in the country were put into action were ambitious.
The mission statement of the NRHM details these as: reduction in the Infant Mortality Rate (IMR) and Maternal Mortality Ratio (MMR), universal access to public health services such as women’s health, child health, water, sanitation and hygiene, immunisation, nutrition, prevention and control of communicable and non-communicable diseases (including locally endemic diseases), access to integrated comprehensive primary healthcare, population stabilisation, gender and demographic balance, revitalisation of local health traditions and the promotion of a healthy lifestyle.
Each of these goals reiterates that health indicators in India at the time (2005-06) were abysmally poor — as poor as access to primary healthcare itself. This was after the Supreme Court had held in multiple judgments that the Right to Health — and as an extension, medical aid to every person and welfare of the public at large — falls under the obligations of the State and is very much considered a part of Article 21, which is the Right to Life.
Rosamma Chechi was among the thousands across the country who became the first batch of women to set out to turn this difficult dream into a reality.
Close to two decades since ASHA workers became delivery points of the system, in the state of Kerala, where Rosamma Chechi and her colleagues were on strike, the MMR and IMR are the lowest in the country.
All kinds of medical specialists have been acknowledged as reasons for the accomplishment of this feat in primary healthcare, except the ASHA workers themselves.
Sulekha, 70, is one among many who has seen Rosamma Chechi and other ASHA workers since they first stepped into the shoes of healthcare workers.

“We owe our wellbeing to them. If I were well, I would be at the strike with all of them,” said Sulekha, as Rosamma Chechi handed iron and folic tablets to her granddaughter. Sulekha recollected how the health of girls and women in her village was one of the ASHA workers’ main areas of focus when they started off.
The mandate from the very beginning had been to combat the high MMR and IMR, and to channel the Integrated Child Development Services in combating malnutrition among the marginalised and poor. They also had to battle the rates of female infanticide, and create a space for acceptance of infant girls.
The mapping of pregnant mothers starts with the ASHA worker registering them in the medical system by issuing them an antenatal card. During her rounds, as Rosamma Chechi checked on antenatal and postnatal mothers according to the records she maintained, she made it a point to interact with their family members as well, quizzing them on the mother’s nutrition and lifestyle. This, she told me, is done not just to evoke a sense of responsibility among her family members, but also to ensure that they are aware that a representative of the State is present and will show up in the event of mistreatment.
After delivery, the ASHA worker initiated the processes to record the birth of the child with a ‘Road to Health’ card. This card is supposed to track everything related to the child’s health, and kick-start good breastfeeding methods. The ASHA worker explains the vaccination routine to the mother and ensures that the infant is brought in for all in-clinic immunisations according to a set timeline (6 weeks, 9 weeks, 2.5 months, 3.5 months and so on).
The ASHA worker will watch out for the earliest signs of growth-faltering and if she picks up that the child is stunted or seems malnourished, the mother will be further trained on what to do, along with in-clinic consultations at the closest Primary Health Centre (PHC) or Community Health Centre (CHC).
This is also where ICDS and other nutrition schemes such as Antyodaya Anna Yojana come in, as programs to stop under-five mortality will then apply.
There are hundreds of such schemes for primary healthcare but the role of the ASHA worker in facilitating their last-mile delivery is critical.
She explains who is eligible for these schemes and benefits and ensures that the people in question receive these benefits.
If the medical presence of the Indian state is felt across villages in India, it is because of people like Rosamma Chechi; it is because of the ASHA workforce.
Another significant success story is the way in which this workforce has provided primary healthcare support to those suffering from non-communicable diseases and managed the spread of communicable diseases across India. In Kerala, where KAHWA held strikes for 260+ days, health scares from the Coronavirus to the Nipah virus have been thwarted by the ASHA workers’ vigilant door-to-door monitoring.
But after fuelling India’s revolution in making primary healthcare accessible, community health workers such as Rosamma Chechi have been left in the lurch.
***
It is day 181 of the strike at Thiruvananthapuram by the KAHWA. A press conference is underway. Questions are being asked and clarifications issued. Suddenly, a middle-aged man, purportedly a senior journalist from a media organisation, grabs the mic and aggressively asks, “Why aren’t y’all protesting in Delhi? Isn’t the problem here the central government?”

Anger rippled through the assembled workers. The journalist felt like a symbol of the system that refused to engage with the group meaningfully, even indulging in character assassination of some of the leaders of KAHWA. One of these leaders is Mini Chechi, a prominent face at the strike site. She calmly picked up the mic.
“You ask this question almost six months into the strike. Aren’t you embarrassed?” she asked him, moving on to explain like one would to a child. “No, the responsibility of paying the minimum wage to an ASHA worker is as much a responsibility of the State as of the Central government. Passing the baton from one to the other and hiding information about promised hikes is telling of how these thousands of ASHA workers and their wellbeing seem inconsequential to all governments.”
Among South Asian countries, India pays its ASHAs the lowest and Pakistan, the highest. The women of the Lady Health Workers Programme in Pakistan are considered government employees with benefits such as paid sick leave and pensions. In Bangladesh, Shashtya Shebikas (also women healthcare workers) receive even better incentives, such as preferential access to loans and healthcare services. It is the same in Nepal.
India does not pay its women healthcare workers even a quarter of what Pakistan, Bangladesh or Nepal pay theirs.
***
“Ah, Rosamma Chechi, all good? I saw you on TV yesterday!” said an auto driver as he drove past us, waving and smiling as widely as Rosamma Chechi does. Everybody we passed as we made our way to patients in Rosamma Chechi’s jurisdiction wanted to stop and talk, giving us their view on the KAHWA strike and asking whether there had been any changes. Chechi spoke to all of them in the same kind tone, but also moved ahead swiftly.

We had 19 patients to visit that day, their locations spread across difficult terrain, as rain poured down in intervals. Each time we felt the droplets, Chechi would open her umbrella in a matter of seconds, giving us both refuge. We couldn’t stop walking else it would be difficult to see all the patients.
The work of an ASHA is spread across the week, with each day allotted a different activity. One day for palliative care, one day for non-communicable disease (NCD) outreach, one day for taking people with communicable diseases to the CHCs or PHCs, one day for the universal immunisation program, one day to be spent each at the women’s wellness clinics and help desks at the CHC/PHC. Apart from these set tasks, there are lists and lists of duties pertaining to scheme outreach, mapping and data collection, which each ASHA has to perform.
Rosamma Chechi managed to do all of this while emerging as one of the key leaders to represent KAHWA during this historic action.
The strike is unprecedented not just because of its duration, but also because of the resolve of the workers to not relent.

After 266 days, KAHWA decided to end their strike at the Secretariat and instead mobilise at the local level, such as for local self-government elections, where they believe a regular engagement with citizens can continue. They did not celebrate the meagre increase in wages from the Central and State government — Rs. 1000, announced on 1 November alongside multiple other promises, as part of an election campaign.
The ASHA workers refused to cry in front of the media channels assembled that day, instead declaring that their mobilisation would continue in other forms; be it door-to-door or panchayat-to-panchayat, until they won their demands: a raise in compensation from Rs. 7,000 to Rs 21,000 per month, Rs 5,00,000 as a one-time pension benefit and dignified work conditions.
The struggle they are leading can lead to a recognition for years of painstaking work, as work. Rosamma Chechi is convinced their efforts will not go to waste. “Our struggle will win. We are the world’s largest community healthcare workforce and we’ll make history one day. Wait and watch.”
Postscript: As this goes to press, the ASHA Workers’ Union in Karnataka has been protesting for close to a year, demanding an increase in wages. They announced a state-wide strike on February 12, 2026, the third in the span of a year. ASHAs in West Bengal also launched an agitation, with an indefinite cease-work strike from December 23, 2025. Their demands are for a minimum salary of Rs 15,000, better working conditions and primarily, that the government recognises them as healthcare workers by way of regularisation.
-
Greeshma Kuthar is an independent journalist and lawyer based in Chennai, Tamil Nadu.
Priyanka Paul is an artist, writer, and activist from Mumbai, India.
Their work revolves around the themes of social justice, self-exploration, and understanding marginalisation. Paul’s work often uses poetry and comedy to subvert. In their free time, you can find Priyanka drinking copious amounts of iced tea, hoarding zines, and starting fires on the internet.